

INTRODUCTION
Oral disease such as periodontal inflammation due to bacterial accumulation can act as a channel to intestinal bowel disease such as ulcerative colitis and Crohn’s disease.
In this blog we are going to see a detailed link between inflammatory bowel disease and periodontitis.
INFLAMMATORY BOWEL DISEASE (IBD)
Inflammatory bowel disease (IBD) could be a cluster of nosological entities that includes 2 major pathological conditions poignant the gastrointestinal tract (GI):
- Crohn’s disease (CD)
- Ulcerative colitis (UC).
IBD could be a complex malady during which system, genetics, and environmental factors all have a role.
The pathological process of IBD involves genetic and environmental factors, like diet, smoking, stress, and microorganisms, and it's characterised by enteric inflammation and epithelial injury.
Its etiopathological mechanism continues to be unclear, however it's thought to be complex, involving genetic, environmental, microorganism and immune reaction connections to the microbiota.
It will have an effect on the whole gastrointestinal tract, from mouth to anus, primarily involving the small intestine (CD) or the big intestine (UC).
Crohn’s disease (CD) is characterised by phagocyte aggregation, oftentimes forming non-caseating granulomas and transmural inflammation. The terminal small intestine is that the commonest site affected, however the malady will involve any site of the alimentary canal.
Ulcerative colitis (UC) is characterised by a big infiltration of neutrophils among the lamina propria and also the crypts, forming micro-abscesses and superficial tissue layer ulceration. The distal colon is that the most affected region
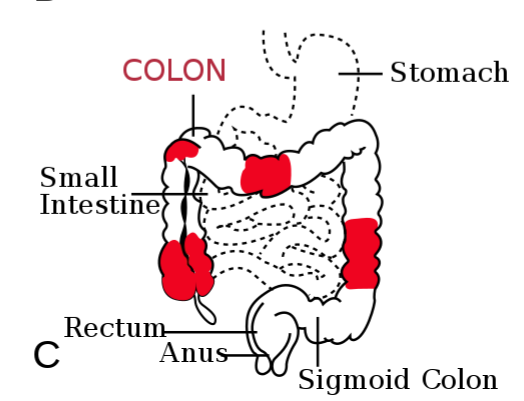
Patterns of Crohn’s disease
Photo credit: Samir, vectorized by Fvasconcellos (Wikipedia commons)
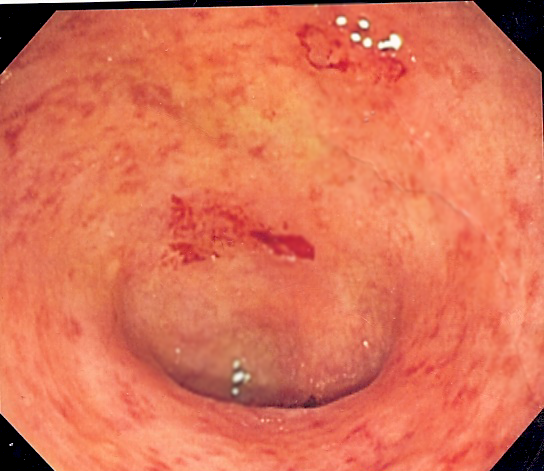
Ulcerative colitis
Red colour patches shows that areas are ulcerated
Photo credit: Kauczuk (Wikipedia commons)
SIGNS AND SYMPTOMS OF UC & CD
Ulcerative colitis
Ulcerative colitis most ordinarily presents as bloody diarrhoea with or while not mucous secretion.
Patients ordinarily describe
- tenesmus
- sensation of incomplete evacuation and
- abdominal pain.
The physical test might reveal preponderantly left lower or left higher quadrant abdominal pain.
Signs of associated acute abdomen as well as guarding, rebound tenderness or percussion tenderness warrant investigation for toxic megacolon.
Crohn's disease
Presentations of Crohn’s disease vary significantly looking at the region of GI involvement.
The symptom complicated of
- right lower quadrant pain
- weight loss and
- non-bloody symptom
are implicational crohn unwellness happening.
Fistula formation might lead to fecaluria, pneumaturia, and rectovaginal fistulas.
Masses within the right lower quadrant counsel associate abscess.
PERIODONTAL DISEASE
Periodontal disease could be a biofilm-induced chronic inflammatory condition that affects the tooth-supporting tissues, that in its severe type could result in tooth loss and negatively have an effect on general health.
Though host immune and inflammatory responses are crucial within the management of this biofilm, their persistence and dysregulation could result in destruction of periodontal tissues, wherever neutrophils and macrophages may play a crucial role.
Moreover, it's been shown that periodontal disease is related to many chronic inflammatory diseases, among that inflammatory bowel disease has raised special attention.
The etiological factors and pathological process of periodontal disease are complex, and developing periodontitis involves each local and general influences.
- Porphyromonas gingivalis
- Aggregatibacter actinomycetemcomitans
- Bacteroides forsythus
- Prevotella intermedia
- Peptostreptococcus micros and
- Fusobacterium nucleatum
are powerfully related to periodontal diseases.
Microorganism colonisation and plaque buildup end in chronic local inflammation, breakdown of barrier, and resultant harm of encompassing gum tissue.
Colonization and growth of microorganisms cause local and general inflammatory responses and destroy the gums, periodontal ligament, or alveolar bone.
Alterations of cytokines in spit or blood serum are ascertained in patients with periodontal disease, as well as IL-1, IL-6, IL-10, IL-17A, IL-17F, IL-22, IL-25, IL-33, tumour necrosis factor-alpha, and interferon-gamma.
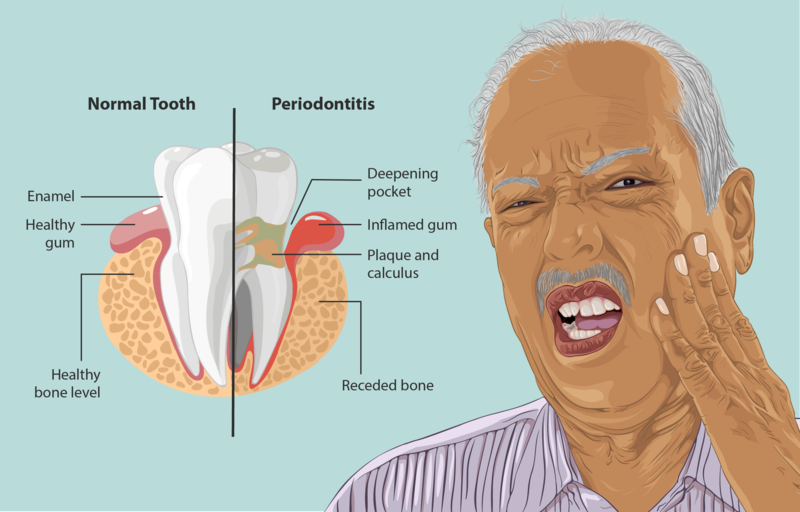
Photo credit: https://www.myupchar.com/en
SIMILARLY BETWEEN PERIODONTAL DISEASE AND INFLAMMATORY BOWEL DISEASE
Microbiome and immune-mediated inflammatory processes play vital roles in each disease, and each has a general impact.
Protein changes were ascertained in each disease and Th1/Th17-related pro-inflammatory cytokines were conjointly concerned within the pathophysiology of those 2 diseases.
They conjointly share similar environmental and lifestyle-related risk factors.
However, the whole mechanism of the accumulated risk isn't totally understood, and also the interactions between these 2 diseases is also bidirectional .
SMOKING AS AN IMPORTANT ETIOLOGICAL FACTOR
Smoking encompasses a totally different impact on the incidence of UC and CD.
Smoking is a very important environmental risk issue and is understood to possess a bearing on IBD.
Individuals who smoke have a higher risk of CD however a lower risk of UC. Smoking could also be protective against UC, and nicotine could have a task within the treatment of UC.
Each innate and adjustive immunity is full of smoking, however the complete mechanism by that smoking exerts its impact on unwellness and therefore the divided impact in patients with CD and UC remains mostly unclear.
Moreover, smoking could also be a potent impact modifier within the interaction between pd and IBD.
PATHOGENESIS OF INFLAMMATORY BOWEL DISEASE BY ORAL PATHOGENS
Large quantities of oral microorganism are perpetually engulfed via the saliva into the gut, it's been projected that engulfed P. gingivalis might cause alterations to the gut microbiota, thereby resulting in augmented gut epithelial porousness and endotoxemia, that causes general inflammation.
Locally created pro-inflammatory cytokines would possibly enter the circulation, induce an acute-phase response within the liver, and contribute to many processes, reminiscent of an arteriosclerosis process.
P. gingivalis, a planned periodontopathogen, evoked changes of microorganism composition of the gut microbiota beside alterations of gut somatic cell barrier function.
TREATMENT OF INFLAMMATORY BOWEL DISEASE
The first step in medical specialty medical care for IBD is aminosalicylates.
If the patient doesn't reply to an applicable dose of aminosalicylates, the second step is the addition of corticosteroids, which tend to lead to a big decrease in inflammation.
Once the response is seen, the dose is tapered.
For those with gentle to moderate disease restricted to the rectum, aminosalicylate agents like mesalamine are mainstays.
Mesalamine is administered rectally however could also be combined with oral medical care to induce or maintain remission.
For those patients with the moderate illness who are refractory to mescaline, oral glucocorticoids or immunomodulators like TNF-a monoclonal antibodies (infliximab) could also be a possibility.
For additional intensive unwellness, general steroid medical care with prednisone is important.
The goal is to wean these steroids among six weeks.
In those patients who cannot wean, associate immunomodulating agents are adscititious.
- 6-mercaptopurine (Purinethol)
- azathioprine (Imuran) or
- low-dose methotrexate sodium.
In those patients with moderate to severe unwellness, anti-tumor necrosis factor (anti-TNF) ought to be initiated.
Before initiating biological medical care, patients should complete sublimate supermolecule by-product (PPD) to assess for latent TB.
PATHOGENESIS OF EXTRAINTESTINAL MALFORMATION (EIM)
The pathologic process of EIMs remains not totally known.
It seems that the inflamed intestinal mucous membrane will trigger immunological responses by sharing common epitopes (e.g., intestinal bacterium and synovia).
Bacterium which will translocate due to larger porosity of the intestinal mucous membrane trigger an non heritable immune reaction that doesn't distinguish between a microorganism epitope and a joint or skin epitope.
In patients with extraintestinal illness manifestations, there's additionally a powerful genetic predisposition.
Extraintestinal complications of inflammatory intestine diseases often occur because of
- malnutrition
- chronic inflammation and
- aspect (side) effects of drugs
which is used to treat IBD

CONSEQUENCES OF IBD IN ORAL LESION AND DISEASES
Malnutrition is present outpatients and hospitalized patients affected by IBD.
It is caused by a
- Reduced food intake
- Reduced reabsorption of nutrients
- Channel losses
- Accrued metabolic needs and
- As a side effect of drugs.
ANEMIA
Anemia could be a common complication of inflammatory viscus malady, which may be manifested in oral pathology.
Iron deficiency is manifested as
- paleness of the oral membrane
- Generalized oral mucosal atrophy
- Pricking
- Atrophic glossitis with tongue pain and
- Angular inflammation.
The deficiency of B vitamin is manifested within the oral fissure as a
- Painful atrophy of the oral membrane and the tongue
- Continual aphthous ulcerations
- Angular cheilitis
- Oral fungal infection
- Diffuse erythroderma redness and pale chromatic membrane, particularly on the roof of the mouth.
Patients may also complain of altered taste, a burning sensation within the mouth and dysphagia.
If anemia is caused by a folic acid deficiency, the manifestations within the oral fissure are an equivalent as in anemia caused by anti pernicious anemia factor deficiency however while not neurologic symptoms.
In more severe cases, lesion redness and raw throat are detected.
VITAMIN DEFICIENCIES
vitamin D deficiency, additionally to disorders within the metabolism of Ca and phosphate in the oral fissure, is among the event of bone hypomineralization and an accrued risk of fractures.
Vitamin D deficiency accrued prevalence of
- Periodontal diseases (gingivitis and periodontitis)
- Tooth decay and
- Tooth loss.
vitamin A deficiency is manifested within the oral fissure as
- Angular inflammation
- Atrophy and xerotes of oral membrane.
The lips are represented as “retreating” as a result of the membrane contracts towards the oral fissure.
vitamin C deficiency is manifested within the oral fissure as
- Generalized gingival swelling and
- Spontaneous hemorrhage
- Ulcerations
- Tooth mobility
- Accrued severity of periodontic infections
- Bone loss.
MEDICATIONS
The medical care applied to treating inflammatory bowel diseases will cause alterations within the mouth due to the direct cyanogenic impact of the drug on the oral tissue, the indirect immunosuppressive result that will increase the danger for opportunistic infections or bone marrow suppression.
corticosteroids
The long-run use of corticosteroids will increase the danger of infection.
The use of those medications is expounded to the prevalence of candidiasis within the mouth, pharynx and oesophagus.
Long-term corticoid use may also end in osteoporosis, moving the patients’ jawbones and increasing the danger of periodontal diseases and fractures.
sulfapyridine
Sulfapyridine and a vigorous substance of 5-aminosalicylic acid (5-ASA)
In the mouth, sulfasalazine causes an oral lichen planus/oral lichenoid reaction.
sulfasalazine could reason for a metallic taste within the mouth.
Azathioprine & 6-mercaptopurine
Azathioprine (AZD) and 6-mercaptopurine (6-MP) are thiopurine medications that are utilized in the treatment of IBD.
AZA has been shown to cause style disturbances within the type of
- ageusia/hypogeusia and
- dysgeusia.
Methotrexate
Methotrexate may be a stomatotoxic drug, that causes oral ulcers, ulcerative stomatitis and mucositis.
Lower doses cause ulcers and rubor.
calcineurin inhibitors (cyclosporine and tacrolimus)
Gingival dysplasia is common in patients receiving cyclosporine (CsA).
Gingival dysplasia can interfere with oral functions and speech and might cause
- delayed and/or posture dentition
- difficulties in maintaining oral hygiene
- increasing the danger of dental caries
- infection and
- periodontitis.
ORAL SPECIFIC LESION AS A INDICATOR FOR
CROHN’S DISEASE(CD)
Dudeney’s report of oral Crohn’s disease in 1969 represented it as a raised, edematous, pink granulation within the buccal mucous membrane.
Oral lesions is also painful, impair correct oral function, or cause psychological disorders because of disfigurement.
Oral manifestations of CD are often specific or non-specific, supported the presence of granulomas noted on the histopathology reports.
The most affected parts within the mouth are the
- buccal mucous membrane
- gingiva
- lips
- vestibular and
- retromolar areas.
white reticulate tags noted as mucosal tags, epithelial tags, or folds.
These lesions are principally discovered within the labial and buccal vestibules, and within the retromolar regions.
Fissured swollen buccal mucous membrane with corrugation and hyperplastic look of the mucosa are referred to as cobblestoning.
These lesions are sometimes seen within the posterior buccal mucous membrane and should be related to succulent tissue layer folds with normal epithelium.
These lesions, along side mucosal tags, are thought-about pathognomonic for CD,but aren't related to intestinal CD activity.
Recurrent aphthous ulcers are common, but it's not clear whether or not this can be because of Crohn’s disease or just that they're common within the general population.
The gingiva might become edematous, granular, and hyperplastic in Crohn’s disease, with or while not ulceration.
The full gingiva up to the mucogingival line could be involved.
Lip swelling with vertical fissures, deep linear ulcerations (usually within the buccal sulci with hyperplastic folds), and plane lip fissuring might also occur in CD.
orofacial granulomatosis (OFG), a rare condition defined by swelling of the lip and also the oral fissure, should be investigated in young kids, as a result of it will conceal underlying Crohn’s malady or be a presenting feature of alternative general diseases.

Aphthous ulcer
Photo credit: TheBlunderbuss (Wikipedia commons)
ORAL NON-SPECIFIC LESION AS A INDICATOR FOR CROHN’S DISEASE(CD)
Non-specific oral findings of CD embrace angular
- cheilitis
- persistent submandibular lymphadenopathy
- sicca syndrome
- reduced salivation
- halitosis
- tooth decay
- periodontic involvement
- monilia disease
- odynophagia
- dysphagia
- minor salivary gland enlargement
- perioral erythroderma with scaling
- repeated buccal abscesses
- glossitis
- mucosal discoloration
- lichen planus and
- gilded dysgeusia.

Glossitis
Photo credit: Martin Kronawitter (Wikipedia commons)
ORAL SPECIFIC LESION AS A INDICATOR FOR
ULCERATIVE COLITIS (UC)
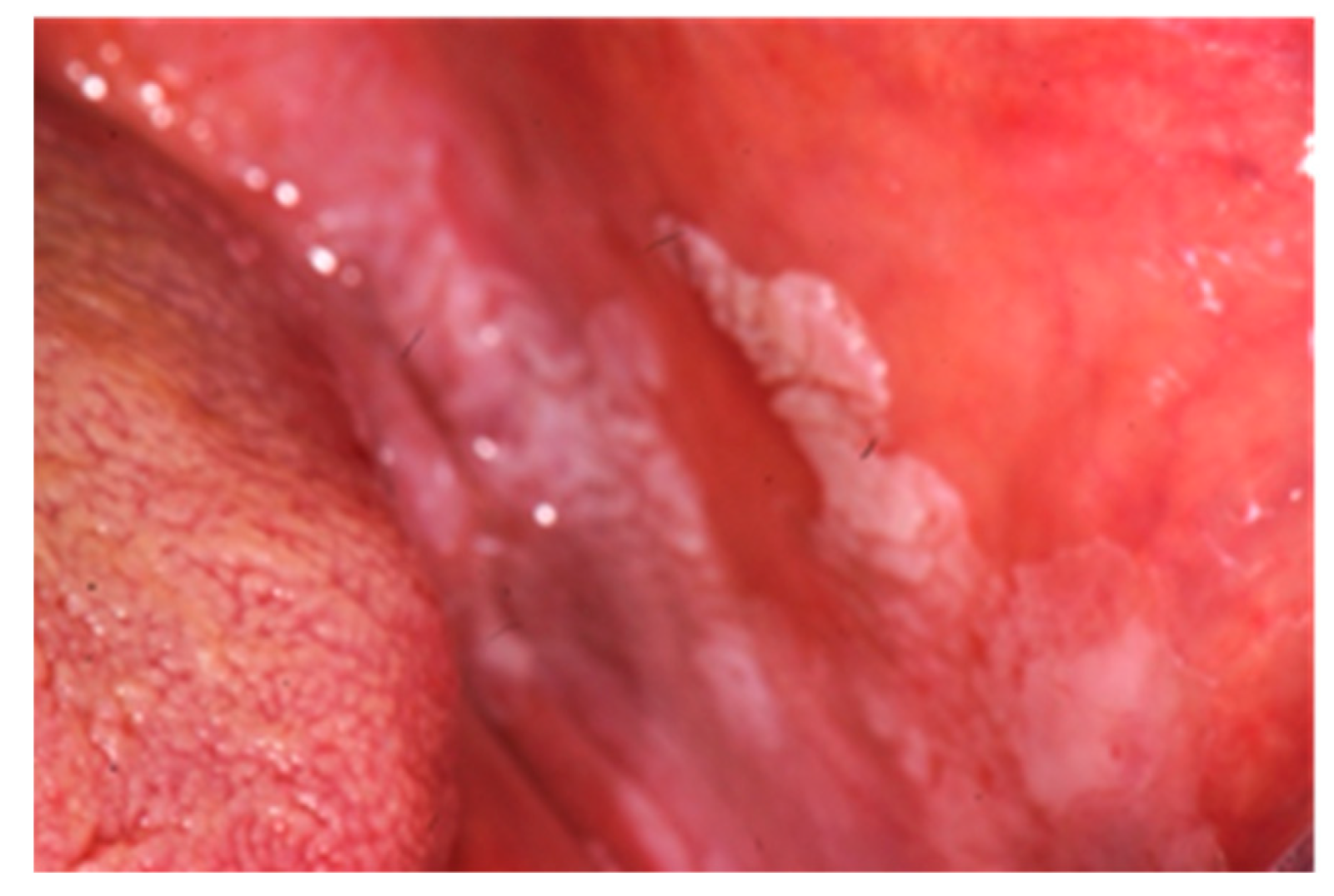
Pyostomatitis vegetans happens additional normally in UC than in CD
The term pyostomatitis vegetans (PV) was initial introduced by McCarthy in 1949.
Pyostomatitis vegetans could be a chronic mucocutaneous lesion disorder consisting of multiple miliary white or yellow pustules with an erythroderma and edematous mucosal base.
The pustules will rupture and coalesce to make linear or “snail-track” ulcers.
The foremost ofttimes concerned regions of the rima oris are the
- labial gingiva
- labial buccal membrane and
- buccal membrane.
Intestinal involvement typically predates the onset of PV in IBD, though this might be symptomless and delicate.
ORAL NON- SPECIFIC LESION AS A INDICATOR FOR ULCERATIVE COLITIS (UC)
Non-specific findings in UC embrace
- oral aphthae
- glossitis
- cheilitis, stomatitis
- lichen
- mucosal ulcers
- diffuse pustules and
- non-specific periodontal disease
Lichen planus
Photo credit: https://doi.org/10.3390/diagnostics9030077
TREATMENT OF THESE ORAL LESIONS
There is sometimes no want for specific treatment for these lesions, however once indicated it's going to comprise
- topical and general steroids
- immunosuppressive drugs
- antibiotics and
- biological treatment in additional severe cases.
For angular cheilitis, 5-ASA mouthwashes, topical steroids (1% hydrocortisone), nourishment supplements, and intra-lesional steroids will be used.
In more severe cases, immunomodulating agents as well as chimerical anti-tissue necrosis factor (TNF) alpha being antibody-infliximab, methotrexate sodium, and sedative-hypnotic are used.
Calcineurin blockers additionally been used dor pyostomatitis vegetans.
Surgical colectomy will be drained pyostomatitis vegetans related to inflammatory bowel disease.
methotrexate are additionally effective, particularly in Pyostomatitis vegetans related to Crohn's disease.
CONCLUSION
The cooperation of each gastroenterologist and dentist is crucial so as to attain early designation, higher management of therapies, and improve patients’ quality of life.
Thus concluding with a quote
"IF YOU TAKE CARE OF YOUR ORAL HEALTH IT WILL AUTOMATICALLY TAKE CARE OF YOUR INTESTINAL HEALTH"
REFERENCE
- Dorina Lauritano, Elisa Boccalari, Dario Di Stasio, Fedora Della Vella, Francesco Carinci, Alberta Lucchese, and Massimo Petruzzi. Prevalence of Oral Lesions and Correlation with Intestinal Symptoms of Inflammatory Bowel Disease: A Systematic Review. Diagnostics (Basel). 2019 Sep; 9(3): 77.
- Ronaldo Lira-Junior, Carlos Marcelo Figueredo. Periodontal and inflammatory bowel diseases: Is there evidence of complex pathogenic interactions?.World J Gastroenterol. 2016 Sep 21; 22(35): 7963–7972.
- McDowell C, Farooq U, Haseeb M. Inflammatory Bowel Disease (IBD) [Updated 2020 Jun 28]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2020 Jan-.
- Chien-Yu Lin,Kuo-Sen Tseng,Jui-Ming Liu,Heng-Chang Chuang,Chi-Hone Lien,Yi-Chih Chen,Chun-Ying Lai,Cheng-Ping Yuand Ren-Jun Hsu. Increased Risk of Ulcerative Colitis in Patients with Periodontal Disease: A Nationwide Population-Based Cohort Study. Int J Environ Res Public Health. 2018 Nov; 15(11): 2602.
- www.wikipedia.com
- Kamran B Lankarani, Gholam Reza Sivandzadeh, and Shima Hassanpour. Oral manifestation in inflammatory bowel disease: A review. World J Gastroenterol. 2013 Dec 14; 19(46): 8571–8579. Baishideng Publishing Group Inc.
- Miranda Muhvić-Urek, Marija Tomac-Stojmenović, and Brankica Mijandrušić-Sinčić. Oral pathology in inflammatory bowel disease. World J Gastroenterol. 2016 Jul 7; 22(25): 5655–5667.Baishideng Publishing Group Inc.
- Dudeney TP. Crohn’s disease of the mouth. Proc R Soc Med. 1969;62:1237.
- Photo credit
- Wikipedia commons
- Pixabay
Your comments are always welcome.. If you have any suggestions or queries please feel free to contact us.








0 Comments